Tracking the progress of labor helps prevent and detect potential complications. Monitoring the characteristics and duration of the different stages of labor, observation, accompaniment of the woman and the control of fetal well-being favor the early diagnosis of complications that may require obstetric intervention.
Different tools are used to track this:
Partogram
It is a tool used to evaluate the progression of labor through a graphical representation of the factors involved: maternal constants (blood pressure, pulse and temperature), fetal heart rate, fetal position relative to the maternal pelvis, characteristics of the waters (quantity, color and odor), the evolution of dilation and uterine dynamics (frequency and intensity of contractions).
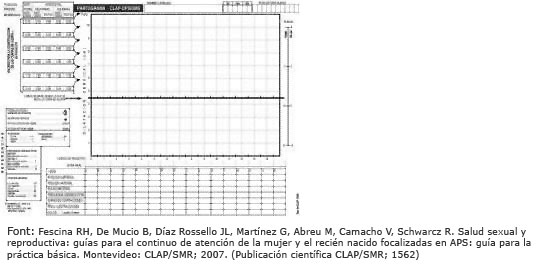
'Partogram', d'Virtual Nurse, content under license CC BY-NC-ND 3.0 ES, with modifications made by the Gynecology and Obstetrics Service of the Hospital de Sabadell
Control of fetal well-being and uterine dynamics
An indirect signal that allows you to know the state of oxygenation and fetal vitality during childbirth is fetal heart rate monitoring (FCF). contractions at the FCF.
Methods for controlling FCF and uterine dynamics:
- Pinard stethoscope. It is a cone-like device, the widest part of which is placed directly on the mother's abdomen, and with her ear at the other end the fetal heartbeat can be heard directly.
- Pinard stethoscope

Source: Lucia Alcaraz and Julia Cid
- Manual control of uterine dynamics. He puts his hand on the woman's abdomen to perceive the duration, frequency and intensity of the contractions.
- Manual Doppler Fetal Monitor. Thanks to ultrasound, the fetal heartbeat can be heard through a probe over the anointed abdomen with conductive gel. This monitor has the advantage that the mother can hear the heartbeat as well.

Source: Lucia Alcaraz and Julia Cid
-
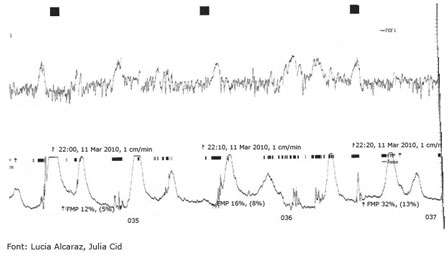
Cardiotocographic record (RCTG) or cardiotocography. It allows you to monitor FCF and uterine dynamics (the intensity and frequency of contractions) continuously and record both data in a graph. The cardiotocographic record can be:
-
External Two electrodes are placed on the maternal abdomen, one with conductive gel to record the FCF and the other to record the presence and duration of contractions. These electrodes are attached to the abdomen with elastic straps and connected to a monitor using two cables or a wireless connection.

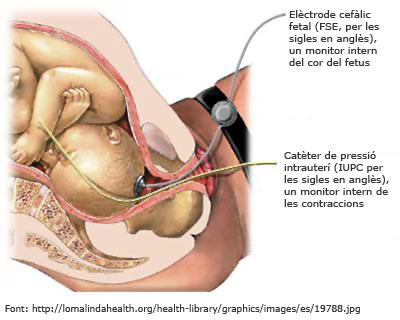
-
Internal An electrode, which is used to indicate FCF, is placed on the fetal head through the vagina and a pressure sensor inside the uterus to capture the uterine contractions. Both sensors are connected to the monitor. Internal cardiotocographic recording should only be used when external cardiotocography is not possible or the information you provide is doubtful.
-
External Two electrodes are placed on the maternal abdomen, one with conductive gel to record the FCF and the other to record the presence and duration of contractions. These electrodes are attached to the abdomen with elastic straps and connected to a monitor using two cables or a wireless connection.
FCF and uterine dynamics can be monitored intermittently or continuously.
-
Intermittent fetal auscultation. It is recommended in women without risk factors. Intermittent auscultation can be performed at different frequencies, such as:
- at least one full minute after contraction, every 15 minutes during the dilation phase and every 5 minutes during expulsion;
- intermittent fetal monitoring lasting 20 minutes every hour during the dilation phase;
- 20 minutes every hour during the dilation phase and after each contraction in the expulsive period.
Intermittent control of contractions can be performed manually or with the external cardiotocographic record.
Intermittent auscultation should be replaced by continuous auscultation if there are any alterations in the FCF or in the development of labor.
-
Continuous monitoring. This system controls the fetal heartbeat and uterine dynamics at all times, without interruption. It is indicated for women and fetuses with any of the following risk factors:
- maternal factors: pathology, previous uterine surgery, etc .;
- fetal factors: meconium water, growth retardation, etc .;
- peridural anesthesia;
- utilization of oxytocin;
- alterations in FCF detected with intermittent auscultation.
Continuous monitoring can be done through an external or internal cardiotocographic record.
It should be borne in mind that continuous monitoring hinders the woman's ability to wander and move freely during labor and may interfere with the process. To improve this, some hospitals may use external wireless monitoring (the signal reaches the monitor by radio frequency).
'Control of fetal well-being and uterine dynamics', d'Virtual Nurse, content under license CC BY-NC-ND 3.0 ES, with modifications made by the Gynecology and Obstetrics Service of the Hospital de Sabadell
Fetal blood micro-extraction (fetal pH)
It is a technique that is performed when the cardiotocographic record is not reassuring. It serves to objectively verify the oxygenation of the fetus from a blood test. The sample is taken through the vagina with a small sting on the fetal scalp.
'Fetal blood micro-extraction (fetal pH)', d'Virtual Nurse, content under license CC BY-NC-ND 3.0 ES, with modifications made by the Gynecology and Obstetrics Service of the Hospital de Sabadell
Control of maternal well-being
Maternal vital signs are regularly evaluated for physical and emotional status. It is recommended to measure your heart rate every hour and your blood pressure and body temperature every four hours. If the woman is under the effects ofepidural anesthesia, you should also be careful that your urine bladder is not full, and recommend urinating if you feel like it or emptying your bladder regularly through a non-permanent bladder.
To favor one optimal maternal well-being You need to ensure proper hydration, a pleasant physical environment, with the right temperature, and an atmosphere of privacy and privacy in which the woman can feel safe and accompanied by the people she wants.
Observing and monitoring a woman are important tools for assessing labor progress: changes in position, ability to concentrate on herself or the sounds she makes are indirect signals to childbirth.
'Maternal welfare control', d'Virtual Nurse, content under license CC BY-NC-ND 3.0 ES, with modifications made by the Gynecology and Obstetrics Service of the Hospital de Sabadell
Vaginal touch
The most commonly used method for assessing the progression of labor is vaginal touch. It is an exploration that involves inserting, with gloved, the index and heart fingers into the vagina to the cervix, in order to evaluate the characteristics of the fetal head (position in relation to the maternal pelvis, degree of reduction and rotation) and of the cervix (position, consistency, length and dilation).
It is advisable to limit the number of touches as much as possible, because they are painful and carry a risk of infection, especially in women who have broken the pouch before the contractions begin.
'Vaginal touch', d'Virtual Nurse, content under license CC BY-NC-ND 3.0 ES